Patient Presentation
A 13-year-old female came to clinic with a 2 week history of “tailbone” pain. It was chronic but not increasing and occurred only during the day. The pain was worse with movement, particularly twisting and lying down. She denied any radiation or shooting pain, nor problems walking or tripping, and no bowel or bladder problems. She also denied any fever, chills, weight loss, bruising or bleeding. There was no trauma and she denied sitting for long periods of time in one position. There were no unusual stressors and she had been going to school and doing social activities. As it was autumn, she was recently raking leaves and doing more outdoor yard work. She had tried occasional ibuprofen with some relief. The past medical history and review of systems were negative. The family history was negative for significant musculoskeletal, neurological or oncological problems.
The pertinent physical exam showed she had appropriate growth parameters with no weight loss and was in mild pain when moving between the chair and examination table. Musculoskeletal examination found pain on the right paraspinal region in the L5-S1 area. The pain became worse with moving to a lying position or hyperextension. It was not changed with flexion. Hips were normal. There was good tone and strength, with normal deep tendon reflexes and normal sensation in the lower extremities. Because of the increased pain with hyperextension, the physician thought that this could be a spondylolysis but the radiologic evaluation of lower spine radiographs were negative. The diagnosis of mechanical back pain was made. She was to begin anti-inflammatory doses of ibuprofen and rest her back for 5 days. If there was no improvement at that time, she was to call back and a referral to physical therapy for back rehabilitation made.

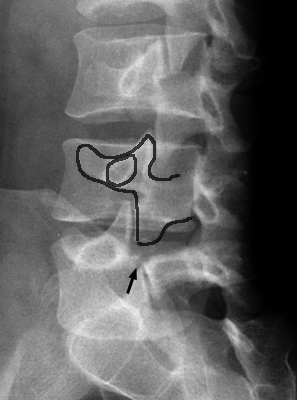
Figure 91 – Oblique radiographs of the lumbar spine demonstrates normal appearing pars interarticularis bilaterally. No scotty dog deformity is noted.
Discussion
Musculoskeletal complaints are common problems but back pain is less common, although probably very much underreported. Back pain is less common in younger children and then increases over time. One study of 1000 consecutive general pediatric clinic visits in patients 3-15 years, found 4 patients presenting with back pain (0.4%), this represented 6% of all patients with musculoskeletal problems. Another study of a population based cohort of children, ages 11-14 years, found a baseline one-month prevalence of 24%. After one year an additional 18.6% reported back pain. Incidence increased with age, female gender, and patients with conduct disorders or increased somatic complaints. Interestingly, backpack weight did not affect the risk of developing back pain. Females may be at increased risk because of different biomechanics including broader hips, greater femoral neck anteversion, and shorter limb length. Pregnancy may also cause stretching of the pelvic and sacroiliac ligaments which could possibly lead to dysfunction.
Back pain is less common in younger children and then increases over time. Therefore the younger the child presenting with back pain, the more likely that it is caused by a serious problem and needs investigation.
Spondylolysis (remember lysis) is a stress fracture of one of the pars interarticularis of the vertebrae usually in the lumbar area. It is often seen in gynmnasts and football lineman, and other sports with repeated hyperextension of the lower back. Oblique radiographs of the lower spine show a “Scotty Dog” appearance. The neck of the Scotty Dog is the pars interarticularis and if there is a “collar” on the dog, then the fracture diagnosis is made.
{kind=link}
Spondylolisthesis is an anterior displacement of the vertebral pedicle often due to bilateral spondylolysis. Spondylolisthesis means vertebral slippage (remember slippage). Therefore with bilateral spondylolysis or bilateral fractures the vertebral pedicle ‘slips’ anteriorly. With spondylolysis or spondylolisthesis, the patient will usually complain of increased pain with hyperextension of the lower spine.
Learning Point
The differential diagnosis of back pain in children includes:
- Musculoskeletal
- Mechanical pain
- Recognized trauma – motor vehicle accident, fall, twisting/lifting heavy object
- Unrecognized trauma – sitting for long time i.e. bicycling, playing an instrument), operating vibratory equipment
- Overuse
- Fracture – hip, spondylolysis, spondylolisthesis
- Vertebral slipped epiphysis
- Arthritis – Juvenile rheumatoid arthritis, ankylosing spondylitis, spondyloarthropathy, Reiter syndrome
- Avascular necrosis of the femoral head
- Disc disease
- Hip disease
- Lumbosacral radiculopathy
- Iliotibial band syndrome
- Sacroilitis
- Mechanical pain
- Infectious
- Osteomyelitis – Staphylococcus, Streptococcus, Tuberculosis
- Sacroiliac joint infection
- Malignancy
- Primary – often spinal cord tumor, less commonly primary bone tumor
- Metastatic – also less common from distant sites but drop metastases from brain tumors may occur
- Other
- Abdominal disease
- Crohn’s disease
- Genetic – congenital or metabolic
- Psychiatric – depression, drug seeking, conversion disorder, malingering
- Sickle cell disease
Questions for Further Discussion
1. What signs or symptoms make serious organic pathology more likely in children?
2. What evaluation can be considered to work-up back pain?
Related Cases
- Disease: Back Pain | Back Injuries
- Symptom/Presentation: Back Pain
- Specialty: General Pediatrics | Orthopaedic Surgery and Sports Medicine | Radiology / Nuclear Medicine / Radiation Oncology
- Age: Teenager
To Learn More
To view pediatric review articles on this topic from the past year check PubMed.
Evidence-based medicine information on this topic can be found at SearchingPediatrics.com, the National Guideline Clearinghouse and the Cochrane Database of Systematic Reviews.
Information prescriptions for patients can be found at MedlinePlus for this topic: Back Pain
To view current news articles on this topic check Google News.
To view images related to this topic check Google Images.
de Inocencio J. Musculoskeletal pain in primary pediatric care: analysis of 1000 consecutive general pediatric clinic visits. Pediatrics. 1998 Dec;102(6):E63.
Jones GT, Watson KD, Silman AJ, Symmons DP, Macfarlane GJ. Predictors of low back pain in British schoolchildren: a population-based prospective cohort study. Pediatrics. 2003 Apr;111(4 Pt 1):822-8.
Sherman AL, Gotlin R. Sacroiliac Joint Injury: Treatment & Medication. eMedicine. Available from the Internet at http://emedicine.medscape.com/article/96054-treatment (rev. 4/28/2008, cited 9/21/2010).
Hills EC, Mechanical Low Back Pain. eMedicine. Available from the Internet at http://emedicine.medscape.com/article/310353-overview (rev. 3/24/2010, cited 9/21/10).
ACGME Competencies Highlighted by Case
1. When interacting with patients and their families, the health care professional communicates effectively and demonstrates caring and respectful behaviors.
2. Essential and accurate information about the patients’ is gathered.
3. Informed decisions about diagnostic and therapeutic interventions based on patient information and preferences, up-to-date scientific evidence, and clinical judgment is made.
4. Patient management plans are developed and carried out.
7. All medical and invasive procedures considered essential for the area of practice are competently performed.
8. Health care services aimed at preventing health problems or maintaining health are provided.
9. Patient-focused care is provided by working with health care professionals, including those from other disciplines.
10. An investigatory and analytic thinking approach to the clinical situation is demonstrated.
11. Basic and clinically supportive sciences appropriate to their discipline are known and applied.
13. Information about other populations of patients, especially the larger population from which this patient is drawn, is obtained and used.
14. Knowledge of study designs and statistical methods to appraisal clinical studies and other information on diagnostic and therapeutic effectiveness is applied.
24. Cost-effective health care and resource allocation that does not compromise quality of care is practiced.
Author
Donna M. D’Alessandro, MD
Professor of Pediatrics, University of Iowa Children’s Hospital